




The Embryo: Development, Quality and Its Role in Fertility Treatment
17.7.2026 · 5 min reading
A lot rides on the first few days after fertilisation — more than most people realise. For couples going through IVF, a good chunk of what determines the outcome is already being decided in that short stretch of time, before a pregnancy has even properly begun. So it is worth knowing what an embryo really is, how it grows, and why the people in the lab keep such a close eye on it.
A lot rides on the first few days after fertilisation — more than most people realise. For couples going through IVF, a good chunk of what determines the outcome is already being decided in that short stretch of time, before a pregnancy has even properly begun. So it is worth knowing what an embryo really is, how it grows, and why the people in the lab keep such a close eye on it.
What Is an Embryo, Exactly?
“Embryo” is the term for the developing organism in roughly the first eight weeks after fertilisation. After that — from about week eight of pregnancy — it becomes a fetus. But in fertility medicine the spotlight falls almost entirely on the earliest part of that window: the handful of days straight after fertilisation, when everything can be watched unfold under the microscope.
The Stages of Embryo Development
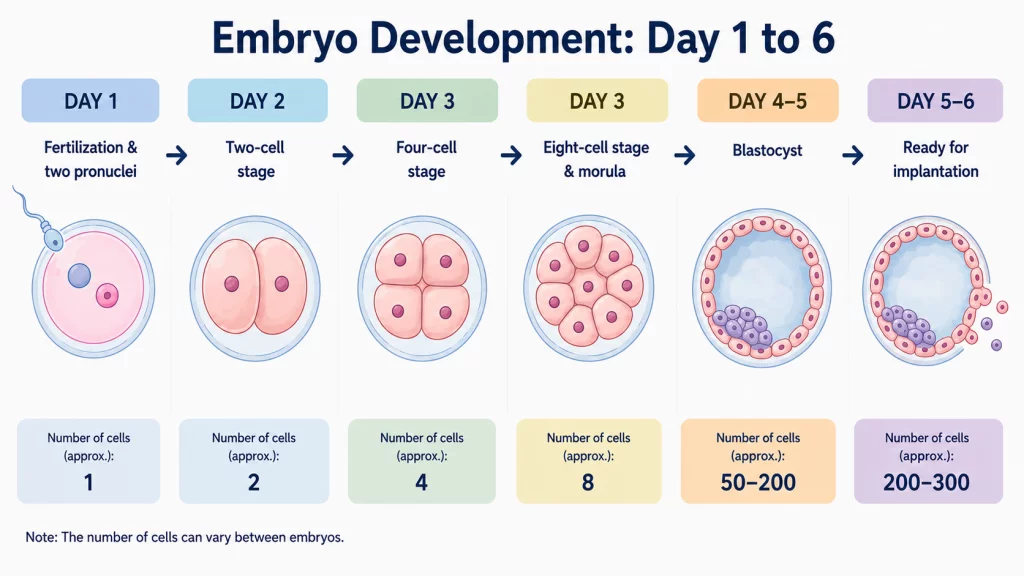
Day 0 to 1: fertilisation and the two pronuclei
Fertilisation is the moment the sperm gets inside the egg. The cell doesn’t waste much time before it starts dividing. A day on, you can make out two structures called pronuclei under the microscope — one carrying the sperm’s genetic material, the other the egg’s. Seeing them is how embryologists know fertilisation has actually worked.
Day 1 to 2: the two-cell stage
By now the embryo has split into two cells, which go by the name blastomeres. Both hold a full set of the genetic material. This is already where the assessing starts — are the cells symmetrical, are they even? Those are the first hints of how good the embryo is.
Day 2 to 3: the four-cell stage
The dividing carries on and you’re now looking at four cells. What you want to see is four cells of much the same size, without bits of fragmented material floating around between them. When an embryo is doing well, the division at this point looks clean and even.
Day 3: the eight-cell stage and the morula
Day three, and ideally the embryo is up to eight cells. Not long after, everything tightens up into a compact little cluster called the morula — a word borrowed from the Latin for mulberry, which is more or less what it looks like. The cells huddle together and start talking to each other, so to speak.
Day 4 to 5: the blastocyst
Somewhere around day four or five the embryo turns into a blastocyst, and this is a big one. For the first time there are two clearly separate parts: the inner cell mass, which goes on to become the baby, and the trophectoderm, which ends up as the placenta. In between sits a cavity filled with fluid — the blastocoel.
Day 5 to 6: ready to implant
Once the blastocyst has swelled out fully and broken free — “hatched”, as it’s called — from its original shell, the zona pellucida, it’s ready to implant. In IVF this is the sweet spot for transferring it back. A good blastocyst at this stage stands a solid chance of taking hold in the uterus.
How Embryo Quality Is Assessed
The grading
Grading comes down to appearance — the morphology, in technical terms. For a blastocyst, three things get the most attention:
- How far it has expanded — the size of the blastocoel and how taut it is
- The inner cell mass, the part the embryo itself grows from
- The trophectoderm, which later becomes the placenta
From there embryos get a grade: A for excellent, down through B and C to D for poor. As a rule, the A’s and B’s are the ones with the strongest odds of implanting and going on to a pregnancy.
Genetic screening: PGT-A
A lot of clinics these days also offer preimplantation genetic testing, PGT-A for short. It looks at the embryo’s chromosomes to catch any abnormalities before transfer. An embryo that’s euploid — meaning it has the right chromosome count — is more likely to lead to a healthy pregnancy.
Embryo Transfer and Implantation
The transfer itself is fairly undramatic. One or more embryos are placed in the uterus through a thin catheter, and there’s usually no anaesthetic involved — it’s a quick, minimal procedure.
When does the transfer happen?
There are two common windows: day three, at the eight-cell stage, or days five to six, once the embryo is a blastocyst. Most clinics lean towards the later one. The success rates are better, and the reason is simple enough — only the hardier embryos make it as far as the blastocyst stage to begin with.
“Not every fertilised embryo makes it to the blastocyst stage — and that is precisely what makes this phase so telling. If an embryo reaches day five or six, it has already shown that it has strong developmental potential.”
— Dr Jana Voborská Neudeckerová
And afterwards?
What follows the transfer is the luteal phase. The embryo now needs to bed into the lining of the uterus, and that typically happens six to ten days out. It’s a good idea to go easy during this time — less stress, no heavy physical exertion.
Common Questions About Embryo Development
Can an embryo develop normally outside the body?
It can. For the first five or six days, embryos grow quite normally in the lab, kept in special culture media designed to copy the conditions inside the body as faithfully as possible.
How many embryos should be transferred?
The trend now is towards a single embryo, particularly for younger women whose outlook is good anyway. Transferring one keeps the odds of a multiple pregnancy down — and twins or more come with a noticeably higher rate of complications.
What are the chances of success?
A few things feed into it: how old the woman is, how good the embryo is, and the state of the uterus. For a top-grade blastocyst in a woman under 35, you’re looking at implantation rates somewhere in the region of 50 to 70% per transfer.
Advances in Embryology
Embryology has moved on considerably in the last few years. Take time-lapse systems: they let the lab keep an unbroken watch on an embryo inside the incubator without ever taking it out and disturbing it. The upshot is a much clearer read on how things are developing — and a better shot at picking out the embryos most worth transferring.
Curious to learn more about embryo development or IVF? Our fertility clinic offers thorough consultations, up-to-date embryology labs and treatment plans built around your particular situation. Alongside IVF, ICSI and IUI, we provide full fertility counselling and egg freezing for those who want to preserve their options. Get in touch and we’ll set up a first appointment.



